I wasn’t familiar with the term “double-stick” when I went through my anesthesia residency. Although we did the typical “big cases” and trauma, we did not routinely place two central lines in a single vein of the same patient. In my current practice, however, it is very common to place two central venous catheters in the IJ for IV access when expecting a large blood loss or a large number of infusions in the ICU.
What is a Double-Stick?
A “double stick” is when you place two central lines into the same vein. This is done fairly commonly by anesthesiologists who care for patients during cases with a chance for rapid blood loss and complex infusions such as liver transplants or cardiac surgery.
It can also refer to when ED physicians access the femoral artery and vein from a single site on a crashing patient. When we say “double stick,” we refer to placing two central lines in the same vein.
Technically it is slightly more difficult to place two central lines vs. one in a single vein, but there are some caveats.
3 Things to consider when performing a double-stick:
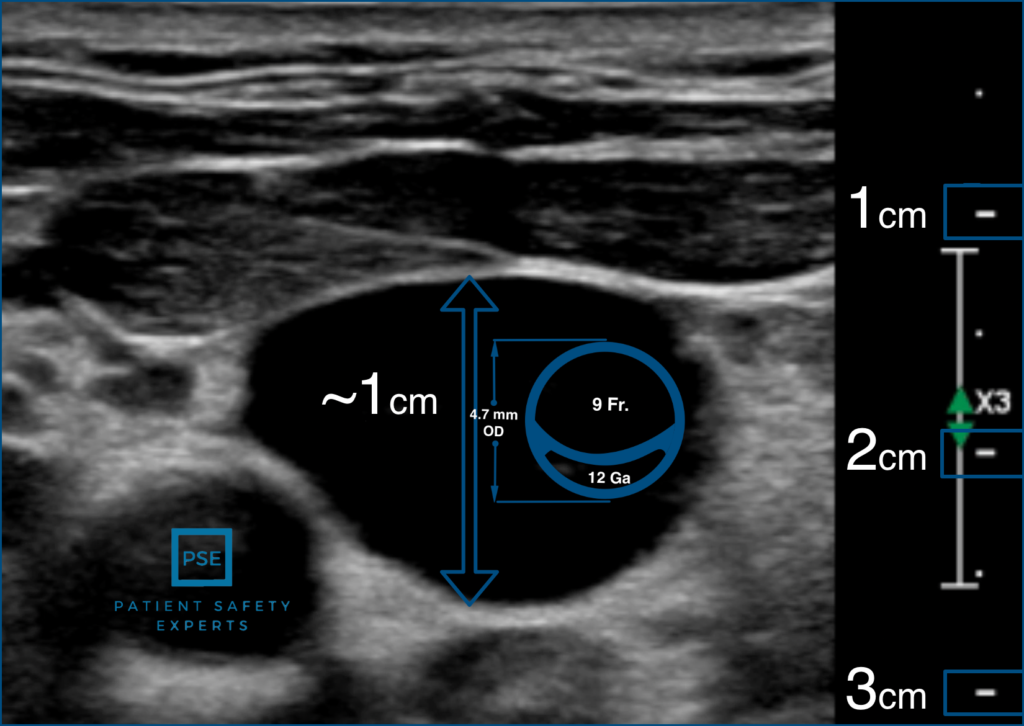
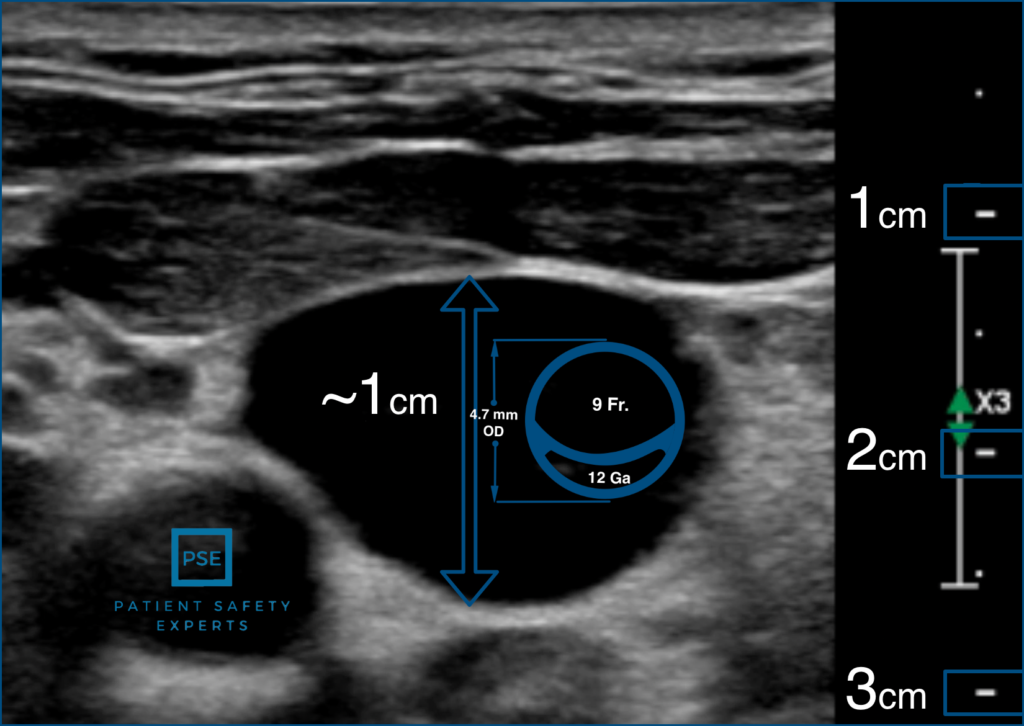
- The vein needs to be large enough to accommodate both catheters. This normally doesn’t present any problems; however, occasionally, if the patient has had a lot of prior lines or is small in stature, the IJ isn’t large enough for two catheters. In the image below you can see that even with a “MAC” line in the IJ, there is still room for a second central line.
- Does the patient have a long or short neck? There are two schools of thought on the double stick. You either place both catheters right next to one another under one dressing, or you try to place them far enough apart that you can place separate dressings on them.
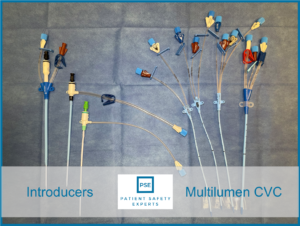
- Which line do you place high, and which do you place low? Which line to place where is subject to much debate in our department. When performing a double-stick, we often combine an introducer with a multi-lumen catheter for either large-bore access or additional ports in the ICU. I prefer to place the introducer higher and turn the multi-lumen catheter lower to act more like a subclavian line.
How much do you really know about central line placement?
Central line insertion is a fundamental skill for all residents, fellows, and attendings. Do you really have the knowledge to be a central line professional?
How to Perform a Double Stick:
Step 1: Scan the neck; decide if the vein is large enough to accommodate two catheters and if you have enough room to place the lines apart or close together.
Step 2: Gain access to the vein, and confirm the venous placement of your first wire
Step 3: Gain access to the vein, and place the second wire.
KEY POINT: When placing your wires, note which wire goes with which line. If you are placing different size catheters, they will have different lengths and diameters of wires.
Step 4: Dilate and place your lower catheter first. Theoretically, this prevents you from damaging the upper catheter if you had placed this catheter first. Carefully remove the wire from the lower catheter. It is VERY easy to pull the wrong wire. You will only make that mistake once!
Step 5: Dilate and place the upper catheter. This should pass easily.
Step 6: Dress your lines carefully. While proper adherence to central line bundles helps prevent CLABSI related to insertion. Getting a good first dressing on the lines helps minimize the need for dressing changes and decreases the risk of CLABSI related to care and maintenance.
This Video Shows How to Perform a Double Stick:
They do not perform manometry to confirm venous placement as we teach.
Is the Double-Stick safe for your patient?
From a technical standpoint, the double stick is slightly more difficult than placing two central lines in different veins. If you have good technique and understand how to use manometry to avoid arterial injury, the double-stick can be used safely.
The real risk to the patient throughout their stay, however, is that patients are at an increased risk of CLABSI if they have two central lines instead of one.
This makes intuitive sense. You have two routes of entry for bacteria to enter the bloodstream. There are twice as many dressings to keep clean and dry. There are more ports to keep disinfected.
My preference today is to minimize the use of a double stick unless one of the lines will be removed shortly after the procedure. My current practice is to place an ultrasound-guided subclavian for my quad lumen central venous catheter for long-term access and easier care and maintenance.
What about you? Do you currently double-stick your central lines?